Asphyxia is a Greek term meaning “stopping of the pulse.” Asphyxial injuries occur when the body is deprived of oxygen, leading to hypoxia and potentially fatal outcomes. The mechanisms of action for asphyxial injuries can be broadly categorized into three main types: respiratory, vascular, and nervous.
Respiratory Mechanism: This involves obstruction or impairment of the airway, preventing oxygen from reaching the lungs. Causes can include choking, strangulation (when the airway is compressed), suffocation, or drowning. The lack of oxygen leads to hypoxia, which can cause brain damage and other organ failures.
Vascular Mechanism: This is the restriction of blood flow to the brain and other vital organs. Traumatic asphyxiation, for example, occurs when a strong external force compresses the thoracic cavity, forcing blood back through the veins to the neck and brain. Strangulation, which involves external compression to the neck, restricts blood flow to the brain.
Nervous Mechanism: The disruption of the nervous system’s ability to regulate breathing. A drug overdose depresses the central nervous system. Injury to the brainstem, the area of the brain that controls respiratory functions.
Asphyxial injuries may be seen in:
Traumatic asphyxiation may be seen in: motor vehicle accidents, industrial accidents where heavy objects/machinery may fall, crowd crushes, building collapses, intentionally inflicted by another person, positional/accidental death
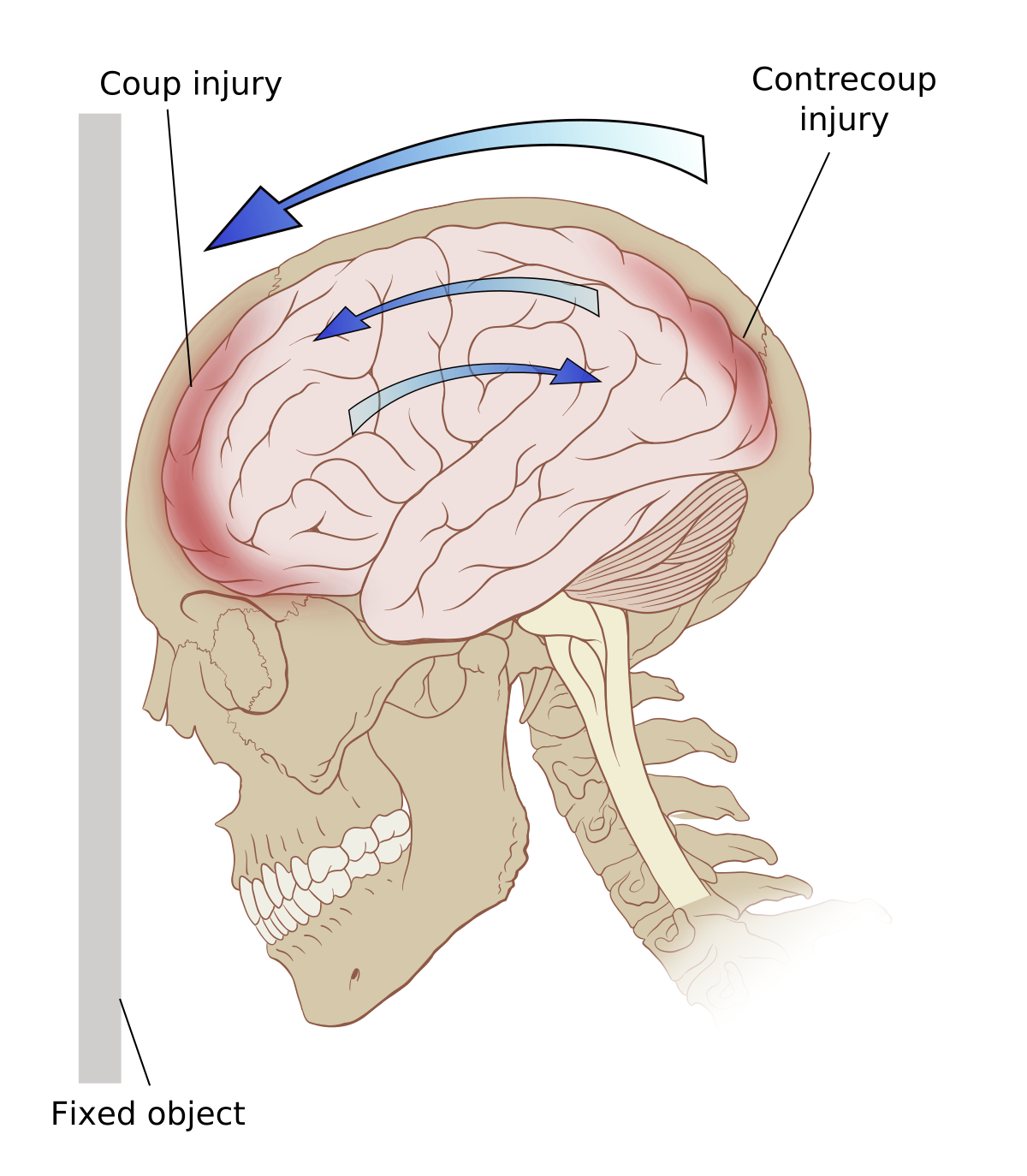
Brain stem injuries may be seen in: motor vehicle/motorcycle accidents, falls, shootings, intentional and accidental blows to the head
Strangulation may be seen in: autoerotic accidents, completed or attempted homicides, suicidal hangings
Smothering may be seen in: attempted/completed homicides, accidental (infants)
Drowning may be seen in: homicide, accident
Deaths from asphyxia may be accidental or intentional (homicide or suicide). Therefore, unless witnessed, many require an autopsy and investigation to rule out foul play. There are several common findings in asphyxial deaths that may be sparsely present, in multiplicity, or not at all:
Congestion of the face due to poor venous return to the heart
Cyanosis due to an excessive lack of oxygen in the venous blood
Facial edema due to increased venous pressure
Petechiae (pinpoint bruising to face, eyes, head, mouth/oral cavity) due to blocked venous flow and increased venous pressure
Injury to skin/soft tissues of head, face, and neck
Internal neck structure damage due to applied force
Airway obstruction, most often by the tongue